Bordetella Pertussis: Why Are Whooping Cough Cases On The Rise?
Author
Chandana Balasubramanian, M.S. ,
30-Dec-2021
Table of Contents
Pathogen of the Month
Whooping cough – an illness that struck fear into the hearts of many during the Great Depression – is back. New Zealanders are being warned about the impending risk of whooping cough and other respiratory infections because of lowered immunity from COVID-19 restrictions [1]. Researchers recently found that immunity against whooping cough is declining among middle-aged adults in many European countries [2].
The World Health Organization (WHO) reports that in 2018, the global burden of pertussis was 151,000 cases. They also confirm that these are often underreported [3]. The United States reported 18,617 pertussis cases in 2019 [4]. In 2015, several provinces in Canada faced pertussis outbreaks, mostly among unvaccinated individuals [5].
Why are pertussis cases growing decades after incidence rates were drastically lowered?
The answer lies in the pathogen’s wily resilience, the fascinating past of the DTP vaccine, and misinformation about the vaccine.
What is Pertussis? How is it Caused?
Pertussis is caused by Bordetella Pertussis, a gram-negative bacterium. Also known as whooping cough, Bordetella is a highly contagious disease. It spreads quickly from person to person through droplets from coughing and sneezing.
Risk factors for this type of Bordetella are:
being unvaccinated, particularly infants and children,
contact with an infected person, and
pregnancy.
People infected with it are highly contagious up to three weeks after their symptoms begin [6].
Symptoms of Pertussis
Pertussis symptoms appear 7 – 10 days after infection. Characteristically, infected individuals have a runny nose, nasal congestion, mild fever, and a severe cough. Many infected individuals or patients also develop pneumonia.
Pertussis is also known as whooping cough because, after a fit of cough, infected people often have to take deep breaths that make a ‘whoop’ sound. It is important to note that not every person or patient with pertussis experiences a whooping sound [3].
Diagnosis of Whooping Cough
A culture is the best way to diagnose whooping cough. This is because many other respiratory infections have the same symptoms. Co-infections like pneumonia are also common. Other tests are PCR and serology [7].
It can be challenging to grow in a laboratory because its growth can be inhibited by many of the laboratory media commonly used. It is fastidious and needs special laboratory media. It also has the slowest growth among all the Bordetella species of bacteria [8].
While Bordetella was historically presumed to be non-flagellated, recent research shows that it can be motile.
Treatment Bordetella Pertussis Infection
The best treatment for this type of Bordetella is a course of antibiotics, delivered early. If treatment is delayed past three weeks of illness, it may be ineffective.
Bordetella Pertussis infection is caused by a human pathogen. It can be very powerful and overcome many of our natural defenses. The bacteria enter the body through the airways and pass down through the respiratory tract. They adhere to the epithelial cells in the trachea and nasopharynx and replicate. In the process, they release toxins that damage the epithelial lining, which induces a severe cough [9]. More specifically the pertussis toxin and the Bordetella pertussis adenylate toxin.
This Bordetella is extremely resilient and has even evolved to evade the immune systems of vaccinated individuals. The bacteria release several toxins, including one that prevents neutrophil cells from entering the infection site. The neutrophils then cannot kill and digest the bacteria, which gives it time to replicate and colonize a larger part of the host’s lungs [10]. These are significant factors that make it hard to treat this Bordetella infection when it is more severe.
Developing the Pertussis Vaccine (DTP): The Fascinating History of 3 Women Who Changed Vaccine Research
An effective vaccination protocol remains the best way to prevent pertussis or whooping cough. Disease rates are highest in regions where vaccination rates are low. In developed countries, pertussis incidence is highest in unvaccinated babies and adolescents.
Before the vaccine, pertussis had a high cumulative incidence, and the mortality rate was one death per ten cases. More children died of pertussis annually in the United States than of polio and measles combined.
The story of the vaccine is that of three women with an uncompromising resolve to help solve the whooping cough crisis in the United States. Pearl Kendrick, Grace Eldering, and Loney Gordon changed the face of vaccine research and clinical study protocols and helped save millions of lives.
“We learned about the disease and the depression at the same time.”
– Grace Eldering, co-developer of the DTP vaccine.
In the 1930s, Pearl Kendrick and Grace Eldering began their whooping cough research project in hopes of creating a vaccination at the Michigan Department of Health laboratory in Grand Rapids, Michigan, USA. Both Kendrick and Eldering had been infected with pertussis as children, and these experiences played a strong role in driving their research. They hired Loney Gordon, an African-American researcher, to support their efforts.
A virulent strain had infected many children in Grand Rapids. Each day, after completing their scheduled laboratory work, Kendrick and Eldering went door to door and collected samples of the pathogen cells from these sick children. They developed strong partnerships with local physicians to get informed about infections and visited poverty-stricken families to collect thousands of samples. This type of field outreach was not common since study protocols were not well-defined at the time.
Using these samples, the women found funding for and ran a large-scale clinical trial during the Great Depression, the longest and worst economic crisis we’ve seen so far, and World War II. Many research studies were severely underfunded and even halted. However, Pearl and Eldering gathered funding from several organizations, including First Lady Eleanor Roosevelt’s Works Progress Administration (WPA). After a three-year trial, the DTP vaccine was declared a success.
Gordon was a significant contributor to the success of the DTP vaccine development. This type of Bordetella is notoriously difficult to grow in a lab. Still, Gordon tested thousands of cultures and identified sheep blood as a critical factor to incubate the culture in a lab. Her research was instrumental in helping Kendrick and Eldering find a strong Bordetella strain effective for the DTP vaccine [11] [12].
This discovery helped them create a rapid cough plate diagnostic tool. Local physicians could send their cough plates to the lab for analysis. This innovation helped the Kendrick-Eldering-Gordon team learn about when a child would be most infectious, the initial three-week infection period. They also figured out that infected children posed no threat to others after five weeks.
This groundbreaking research and the success of the clinical trial helped save the lives of millions of children worldwide. While their clinical trial methodology underwent significant scrutiny from the medical profession, the discussion led to a more robust methodology and protocols.
Even initial skeptics were eventually convinced of the effectiveness of the vaccines. The most prominent of them was Wade Hampton Frost, an epidemiologist from Johns Hopkins University and the head of the American Public Health Association (APHA). While Frost was critical at first, he accepted Kendrick and Eldering’s results [13] [14] [15].
Why Are Pertussis Rates Rising Again?
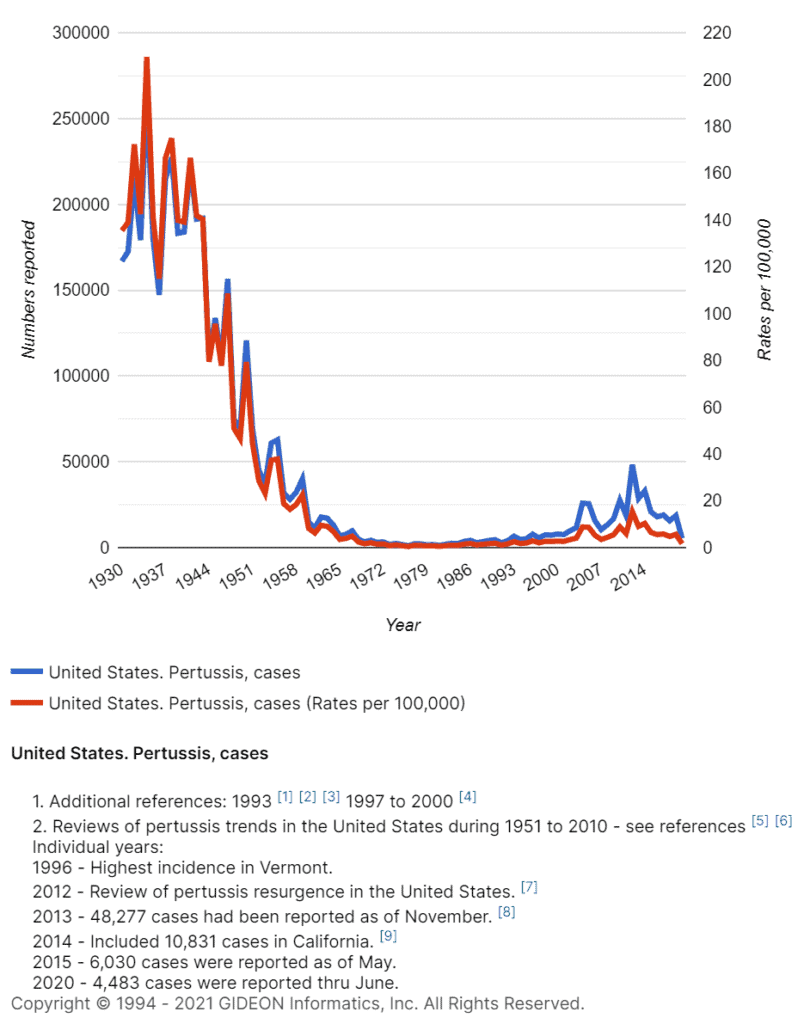
In the 1940s, after the clinical trial for a whole-cell vaccine concluded, the pertussis vaccine was combined with diphtheria andtetanus. The resulting DTP vaccine became commercially available. By 1948, infections of pertussis in the United States dropped drastically (below 100,000). Incidence dropped 75% after the DTP vaccine [16]. If you’re looking to hear more about this, check out this interview on how pertussis is making a comeback.
Image: Chart depicting Pertussis cases in the United States.
Unfortunately, infections began to rise again in the late 1990s. This was because, in 1997, there was a growing public outcry against the rare side effects of the vaccine. Additionally, the vaccine was also blamed for a series of unrelated issues, and many people refused to give the vaccine to their children. As a result, the vaccine was switched to an acellular version DTaP – less effective than whole-cell but with milder side effects.
When the United States, Canada, and many other developed nations made the switch to the DTaP vaccine, the epidemiology of pertussis changed. Instead of affecting much younger children, vaccinated adolescents and school-aged children became infected. Studies are still underway to understand precisely why [17] [18].
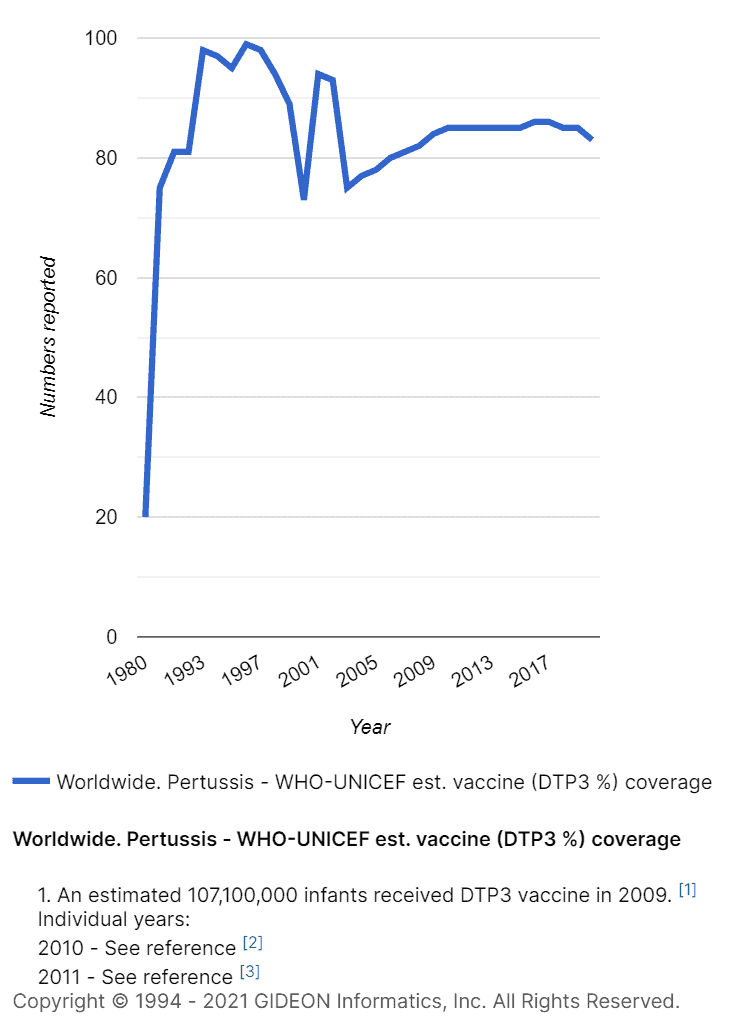
Image: Chart depicting Pertussis cases worldwide.
Pertussis Vaccination Recommendations
The World Health Organization (WHO) recommends a three-dose series of DTP:
The first dose as early as 6 weeks of age.
The rest of the doses given 4-8 weeks apart, at ages 10-14 weeks and 14-18 weeks.
Booster doses are recommended in children aged two.
Additional boosters can also be needed based on the regional epidemiology of the disease [3].
The CDC recommends that all pregnant women receive a TDaP vaccine during the 27th – 36th week of each pregnancy, preferably in the earlier part of this period [19].
Children, infants, and pregnant women are advised to get the vaccine. Babies are most vulnerable and cannot build their immunity against disease-causing pathogens until they are vaccinated. When women are vaccinated during their third trimester, antibodies can be passed on to their babies in utero when they are at the highest risk.
Curbing the Spread of Pertussis
With the COVID-19 pandemic, many routine vaccine programs were suspended. Unfortunately, WHO and UNICEF estimate that, globally, 23 million children did not receive basic childhood vaccines. This includes DTP and DTaP. In 2020, India had the greatest increase in infants and children who did not receive their first dose. DTP-3 coverage fell from 91% to 85% from 2019 to 2020.
It would be highly devastating for countries already battling COVID-19-related infections to face widespread outbreaks of Diptheria, tetanus, pertussis, measles, and other preventable infections.
Resuming active immunization programs and more research is crucial to help prevent infant and childhood deaths and severe illness from deadly whooping cough.
B. G. e. al, “Circulation of pertussis and poor protection against diphtheria among middle-aged adults in 18 European countries,” Nature Communications, vol. 2871 , 2021.
[3]
World Health Organization, “Pertussis,” WHO, 2021. [Online][Accessed 30 12 2021].
R. R. Hulbert and P. A. Cotter, “Laboratory Maintenance of Bordetella pertussis,” Curr Protoc Microbiol, p. Chapter 4:Unit 4B.1, 2009.
[9]
M. A. Smith, C. A. Guzman and M. J. Walker, “The virulence factors of Bordetella pertussis: a matter of control,” FEMS Microbiology Reviews, vol. 25, no. 3, p. 309–333, 2001.
[10]
G. S. Kirimanjeswara, L. M. Agosto, M. J. Kennett, O. N. Bjornstad, and E. T. Harvill, “Pertussis toxin inhibits neutrophil recruitment to delay antibody-mediated clearance of Bordetella pertussis,” The Journal of Clinical Investigation, vol. 115, no. 12, pp. 3594-3601, 2005.
[11]
Michigan Women Forward, “Loney Clinton Gordon,” MIWF.ORG, 2021. [Online] [Accessed 30 12 2021].
G. Eldering, “Symposium on pertussis immunization, in honor of Dr. Pearl L. Kendrick in her eightieth year: historical notes on pertussis immunization,” Health Lab Sci, vol. 8, no. 4, pp. 200-5, 1971.
[14]
C. G. Shapiro-Shapin, “A Whole Community Working Together”: Pearl Kendrick, Grace Eldering, and the Grand Rapids Pertussis Trials, 1932-1939,” Michigan Historical Review, vol. 33, no. 1, pp. 59-85, 2007.
[15]
C. G. Shapiro-Shapin, “Pearl Kendrick, Grace Eldering, and the Pertussis Vaccine,” Emerg Infect Dis, vol. 16, no. 8, p. 1273–1278, 2010.
N. P. Klein, “Licensed pertussis vaccines in the United States: History and Current State,” Hum Vaccine Immunother, vol. 10, no. 9, p. 2684–2690, 2014.
[18]
J. D. Cherry, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines-Mistakes Made and Implications for the Future,” J Pediatric Infect Dis Soc, vol. 8, no. 4, pp. 334-341, 2019.
Chandana Balasubramanian is an experienced healthcare executive who writes on the intersection of healthcare and technology. She is the President of Global Insight Advisory Network, and has a Masters degree in Biomedical Engineering from the University of Wisconsin-Madison, USA.
This site uses cookies. If you don't mind, just click accept and continue browsing. Accept
Manage consent
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.