History
Historians lack clarity concerning the origins of smallpox. It is believed to have initially appeared in North-Eastern Africa around 10,000 BC [3]. Egyptians’ mummified bodies had rashes, leading some to believe that the disease did exist some 3,000 years ago. However, early clinical descriptions of the condition were documented in China in the 4th century. Scripts describing the disease were also discovered in India and Asia Minor during the 7th and 10th centuries [6].
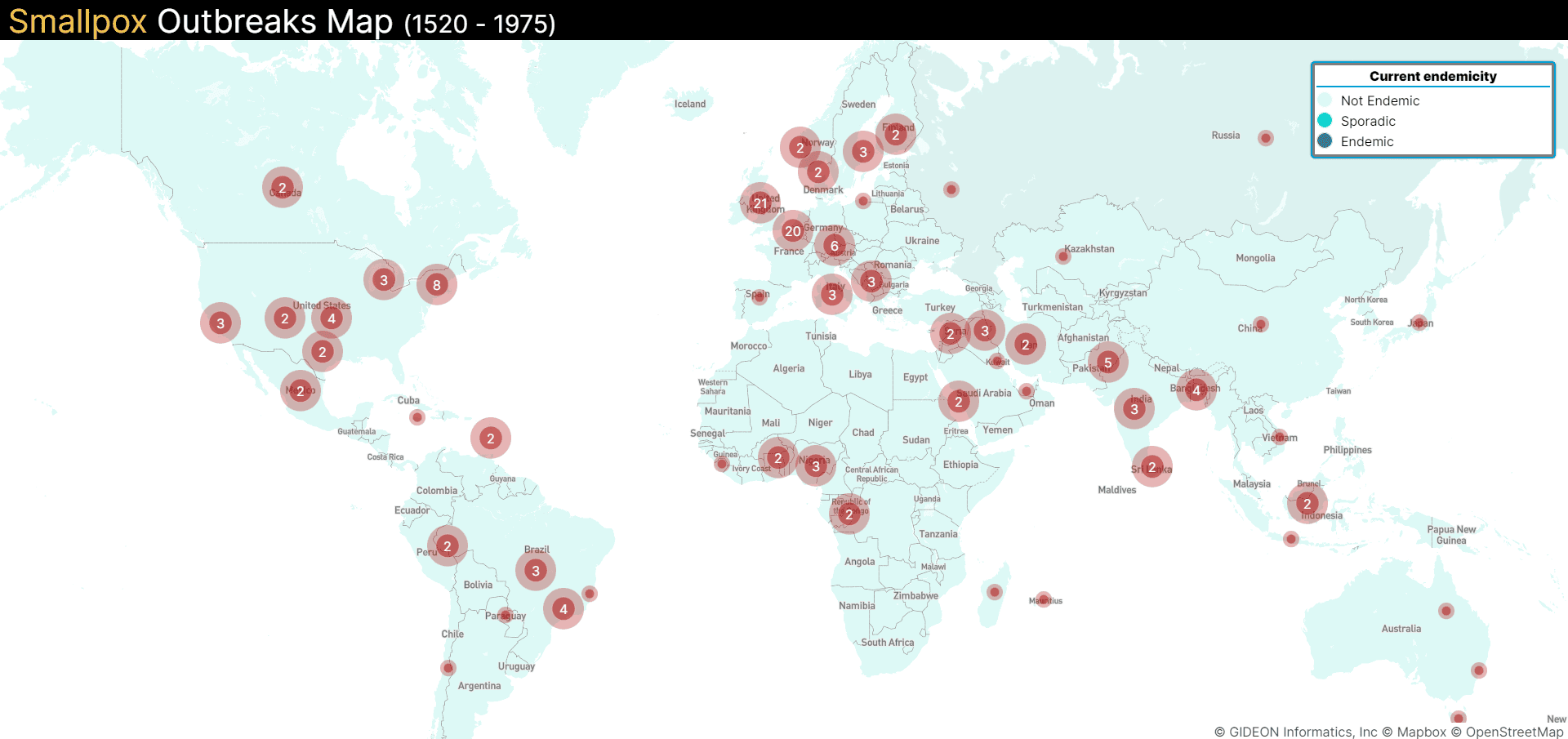
Eventually, wars helped the smallpox virus travel all across the world, bringing widespread illness and fatalities with it. In the 11th century, smallpox began spreading to Europe because of ‘The Crusades,’ a series of religious wars. By the 15th century, smallpox had wandered over to Western Africa, brought to the continent by a colonizing Portuguese military [6]. In the 16th century, the disease spread to the Caribbean and Central and South America, causing widespread devastation [7].
Smallpox did not arrive on American shores until the 17th century. As more Europeans fled their homeland for new shores, smallpox traveled with them to the North American continent [6]. The transatlantic slave trade was another significant factor fueling the smallpox epidemic in America. People from Africa were brought to America in overcrowded and highly unhygienic conditions that served as a hotbed for smallpox and other infectious diseases. Smallpox spread rapidly among Native Americans and decimated their population [3].
The story of smallpox is gruesome. In the 18th century, around 400,000 people died each year in Europe due to smallpox, and nearly one-third of those who survived went blind. During this period, the case fatality rate varied from 20% to as high as 60%. By the end of the 19th century, the infant case fatality rate was extremely high, with 80% in London and 98% in Berlin, Germany — nearly all infants who contracted the disease died [3].
During this period, emerging scientific breakthroughs began to offer hope in the fight against smallpox. In 1796, Dr. Edward Jenner observed that milkmaids who recovered from cowpox were immune to smallpox. This British country doctor is credited with inventing the first smallpox vaccine using the cowpox virus. In 1887, the variola virus was first visualized under a microscope by John B. Buist [8]. Later, in 1935, the pathogen was cultivated for the first time by Torres and Teixeria [8,9].
Although vaccine development efforts started in the 18th and 19th centuries by physicians like Dr. Edward Jenner and Dr. William Osler (the father of Modern Medicine), an effective vaccine was developed only in the 1950s. Encouraged by this development, the World Health Assembly launched its first smallpox eradication campaign in the late 1950s.
At first, the smallpox vaccines were delivered by a large, unwieldy injector which slowed down vaccination drives. However, a bifurcated needle developed in the late 1960s changed the game, allowing for larger-scale vaccination campaigns. The needle was relatively inexpensive and easy to sterilize. It was also simple to use and required very little training, which made mass vaccination drives possible. The needle could hold a small drop of vaccine between its prongs — the ideal amount needed for immunization. This way, vaccine manufacturers could reduce the volume of vaccine required per dose, which meant more people could be vaccinated for the same amount of vaccine produced [10, 22].
The eradication of smallpox is one of humankind’s biggest achievements. The global vaccination effort was unprecedented and involved a concerted effort by many countries. The eradication program was hugely successful, and the last case of smallpox was reported in Bangladesh in 1975. In 1980, smallpox was declared eradicated by the World Health Assembly [10].
Although smallpox had been eradicated, many laboratories continued to stock the variola virus for research. In 1981, the US, the UK, Russia, and South Africa were the only countries involved in variola virus research. By 1984, the UK and South Africa had destroyed most of their stock, leaving behind the US and Russia [6].
Later, evidence of smallpox being developed as a bioweapon in Russia began making news. There were also allegations that Russia was developing more virulent strains of the virus to be used as bioterrorism agents. Many nations were concerned, which led to the development of renewed smallpox vaccinations during the early 2000s [10].